
Acute Appendicitis: Physical Examination

|
EtiologyPathophysiologyHistoryPhysical ExaminationInvestigationsDifferential DiagnosisManagementClinical Scenarios |
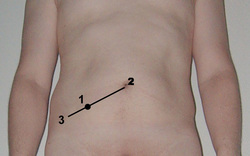
Tenderness on palpation in the right iliac fossa (RIF) over the McBurney's point (Point 1 in the figure) is the most important sign of acute appendicitis.
More specific physical findings in appendicitis are rebound tenderness, pain on percussion, rigidity, and guarding.
Although RIF tenderness is present in 96% of patients, this is a nonspecific finding and can be present in a number of other conditions presenting as acute abdomen.
Accessory signs
In a minority of patients with acute appendicitis, some other signs may be noted. However, their absence should not be used to rule out acute appendicitis.
Rovsing’s sign
(Named after the Danish surgeon Neils Thorkid Rovsing)
It is said to be positive if palpation in the left lower quadrant results in increased pain in the RIF. Posivite Rovsing’s sign suggests peritoneal irritation in the RIF precipitated by palpation at a remote location.
Obturator sign
It is a sign of appendicitis or other peritoneal inflammation and is said to be positive if patient complains of RIF pain with internal rotation of the right leg with the leg flexed to 90 degrees at the hip and knee.
Psoas sign
Right iliac fossa pain with extension of the right hip or with flexion of the right hip against resistance suggests irritation of the ilio psoas group of hip flexors. Positive psoas sign may indicate an inflamed retrocaecal appendix.
Extra Tips: It is important to remember that the position of the appendix is very variable. Of 100 patients undergoing 3-dimensional (3-D) multidetector computed tomography (MDCT) scanning, the base of the appendix was located at the McBurney point in only 4% of patients; in 36%, the base was within 3 cm of the point; in 28%, it was 3-5 cm from that point; and, in 36% of patients, the base of the appendix was more than 5 cm from the McBurney point.
( Ref: Oto A, Ernst RD, Mileski WJ, Nishino TK, Le O, Wolfe GC, et al. Localization of appendix with MDCT and influence of findings on choice of appendectomy incision. AJR Am J Roentgenol. Oct 2006;187(4):987-90)
More specific physical findings in appendicitis are rebound tenderness, pain on percussion, rigidity, and guarding.
Although RIF tenderness is present in 96% of patients, this is a nonspecific finding and can be present in a number of other conditions presenting as acute abdomen.
Accessory signs
In a minority of patients with acute appendicitis, some other signs may be noted. However, their absence should not be used to rule out acute appendicitis.
Rovsing’s sign
(Named after the Danish surgeon Neils Thorkid Rovsing)
It is said to be positive if palpation in the left lower quadrant results in increased pain in the RIF. Posivite Rovsing’s sign suggests peritoneal irritation in the RIF precipitated by palpation at a remote location.
Obturator sign
It is a sign of appendicitis or other peritoneal inflammation and is said to be positive if patient complains of RIF pain with internal rotation of the right leg with the leg flexed to 90 degrees at the hip and knee.
Psoas sign
Right iliac fossa pain with extension of the right hip or with flexion of the right hip against resistance suggests irritation of the ilio psoas group of hip flexors. Positive psoas sign may indicate an inflamed retrocaecal appendix.
Extra Tips: It is important to remember that the position of the appendix is very variable. Of 100 patients undergoing 3-dimensional (3-D) multidetector computed tomography (MDCT) scanning, the base of the appendix was located at the McBurney point in only 4% of patients; in 36%, the base was within 3 cm of the point; in 28%, it was 3-5 cm from that point; and, in 36% of patients, the base of the appendix was more than 5 cm from the McBurney point.
( Ref: Oto A, Ernst RD, Mileski WJ, Nishino TK, Le O, Wolfe GC, et al. Localization of appendix with MDCT and influence of findings on choice of appendectomy incision. AJR Am J Roentgenol. Oct 2006;187(4):987-90)
