
Acute Pancreatitis: Physical Examination
|
The following physical examination findings may be noted, varying with the severity of the disease:
|
EtiologyPathophysiologyHistoryPhysical ExaminationInvestigationsDifferential DiagnosisManagementClinical ScenariosAnswers |
- A minority of patients exhibit jaundice (28%).
- Some patients experience dyspnea (10%), which may be caused by irritation of the diaphragm (resulting from inflammation), pleural effusion, or a more serious condition, such as acute respiratory distress syndrome (ARDS); tachypnea may occur; lung auscultation may reveal basilar rales, especially in the left lung.
- In severe cases, hemodynamic instability is evident (10%) and hematemesis or melena sometimes develops (5%); in addition, patients with severe acute pancreatitis are often pale, diaphoretic, and listless.
- Occasionally, in the extremities, muscular spasm may be noted secondary to hypocalcemia.
A few uncommon physical findings are associated with severe necrotizing pancreatitis:
|
The Cullen Sign is a bluish discoloration around the umbilicus resulting from hemoperitoneum. |

|
|
The Grey-Turner Sign is a reddish-brown discoloration along the flanks resulting from retroperitoneal blood dissecting along tissue planes; more commonly, patients may have a ruddy erythema in the flanks secondary to extravasated pancreatic exudate.
|

|
|
Erythematous skin nodules may result from focal subcutaneous fat necrosis; these are usually not more than 1 cm in size and are typically located on extensor skin surfaces; in addition, polyarthritis is occasionally seen. |

|
Complications
|
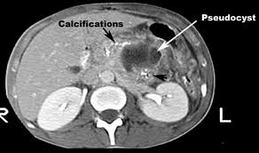
Acute Pseudocyst: This is a collection of pancreatic fluid that is walled off by granulation tissue after an episode of acute pancreatitis; it requires 4 or more weeks to develop. Although pseudocysts are sometimes palpable on physical examination, they are usually detected with abdominal ultrasonography or computed tomography (CT).
|
|
Intra abdominal Infections: Within the first 1-3 weeks, fluid collections or pancreatic necrosis can become infected and jeopardize clinical outcome. From 3 to 6 weeks, pseudocysts may become infected or a pancreatic abscess may develop. The intestinal flora is the predominant source of bacteria causing the infection. The usual suspects are Escherichia coli (26%), Pseudomonas species (16%), Staphylococcus species (15%), Klebsiella species (10%), Proteus species (10%), Streptococcus species (4%), Enterobacter species (3%), and anaerobic organisms (16%). Fungal superinfections may occur weeks or months into the course of severe necrotizing pancreatitis.
Pancreatic necrosis is a nonviable area of pancreatic parenchyma that is often associated with peripancreatic fat necrosis and is principally diagnosed with the aid of dynamic spiral CT scans. Distinguishing between infected and sterile pancreatic necrosis is an ongoing clinical challenge. Sterile pancreatic necrosis is usually treated with aggressive medical management, whereas almost all patients with infected pancreatic necrosis require surgical debridement or percutaneous drainage if they are to survive.
Hemorrhage into the gastrointestinal (GI) tract retroperitoneum or the peritoneal cavity is possible because of erosion of large vessels. Intestinal obstruction or necrosis may occur. Common bile duct obstruction may be caused by a pancreatic abscess, pseudocyst, or biliary stone that caused the pancreatitis. An internal pancreatic fistula from pancreatic duct disruption or a leaking pancreatic pseudocyst may occur.
