
Acute Pancreatitis: Pathophysiogy
|
EtiologyPathophysiologyHistoryPhysical ExaminationInvestigationsDifferential DiagnosisManagementClinical ScenariosAnswers |

Acute pancreatitis occurs when factors involved in maintaining cellular homeostasis are out of balance. The initiating event may be anything that injures the acinar cell and impairs the secretion of zymogen granules; examples include alcohol use, gallstones, and certain drugs.
It is unclear exactly what pathophysiologic event triggers the onset of acute pancreatitis. It is believed, however, that both extracellular factors (eg, neural and vascular response) and intracellular factors (eg, intracellular digestive enzyme activation, increased calcium signaling, and heat shock protein activation) play a role.
Once a cellular injury pattern has been initiated:
· Lysosomal and zymogen granule compartments fuse, enabling activation of trypsinogen to trypsin
· Intracellular trypsin triggers the entire zymogen activation cascade
· Secretory vesicles are extruded across the basolateral membrane into the interstitium, where molecular fragments act as chemoattractants for inflammatory cells
The mediators of inflammation (TNF alpha, IL6, IL 8) cause an increased pancreatic vascular permeability, leading to hemorrhage, edema, and eventually pancreatic necrosis. As the mediators are excreted into the circulation, systemic complications can arise, such as bacteremia due to gut flora translocation, acute respiratory distress syndrome (ARDS), pleural effusions, gastrointestinal (GI) hemorrhage, and renal failure.
The systemic inflammatory response syndrome (SIRS) can also develop, leading to the development of systemic shock. Eventually, the mediators of inflammation can become so overwhelming to the body that hemodynamic instability and death ensue.
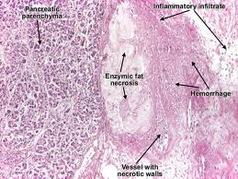
In acute pancreatitis, parenchymal edema and peripancreatic fat necrosis occur first; this is known as acute edematous pancreatitis. When necrosis involves the parenchyma, accompanied by hemorrhage and dysfunction of the gland, the inflammation evolves into hemorrhagic or necrotizing pancreatitis. Pseudocysts and pancreatic abscesses can result from necrotizing pancreatitis because enzymes can be walled off by granulation tissue (pseudocyst formation) or via bacterial seeding of pancreatic or peripancreatic tissue (pancreatic abscess formation).
It is unclear exactly what pathophysiologic event triggers the onset of acute pancreatitis. It is believed, however, that both extracellular factors (eg, neural and vascular response) and intracellular factors (eg, intracellular digestive enzyme activation, increased calcium signaling, and heat shock protein activation) play a role.
Once a cellular injury pattern has been initiated:
· Lysosomal and zymogen granule compartments fuse, enabling activation of trypsinogen to trypsin
· Intracellular trypsin triggers the entire zymogen activation cascade
· Secretory vesicles are extruded across the basolateral membrane into the interstitium, where molecular fragments act as chemoattractants for inflammatory cells
The mediators of inflammation (TNF alpha, IL6, IL 8) cause an increased pancreatic vascular permeability, leading to hemorrhage, edema, and eventually pancreatic necrosis. As the mediators are excreted into the circulation, systemic complications can arise, such as bacteremia due to gut flora translocation, acute respiratory distress syndrome (ARDS), pleural effusions, gastrointestinal (GI) hemorrhage, and renal failure.
The systemic inflammatory response syndrome (SIRS) can also develop, leading to the development of systemic shock. Eventually, the mediators of inflammation can become so overwhelming to the body that hemodynamic instability and death ensue.
In acute pancreatitis, parenchymal edema and peripancreatic fat necrosis occur first; this is known as acute edematous pancreatitis. When necrosis involves the parenchyma, accompanied by hemorrhage and dysfunction of the gland, the inflammation evolves into hemorrhagic or necrotizing pancreatitis. Pseudocysts and pancreatic abscesses can result from necrotizing pancreatitis because enzymes can be walled off by granulation tissue (pseudocyst formation) or via bacterial seeding of pancreatic or peripancreatic tissue (pancreatic abscess formation).
